Tongue ties, breastfeeding and ankyloglossia
When yes, when no, and how we decide. The full series on frenectomy in babies and children.
Tongue tie and lip tie are the consultations I receive most often at Bites Odontopediatría. And honestly, many times the answer is don't operate. Ankyloglossia is being over-diagnosed, and by extension, over-treated. The real clinical decision is based on function, not on how the tongue looks. In this series I explain how we evaluate as a multidisciplinary team, which signs matter, which technique we use in each case (scissors, laser or combined) and what recovery looks like.
Dra. Florencia Nogueira, Pediatric dentist · Bites Odontopediatría
What this topic covers
Frequently asked questions
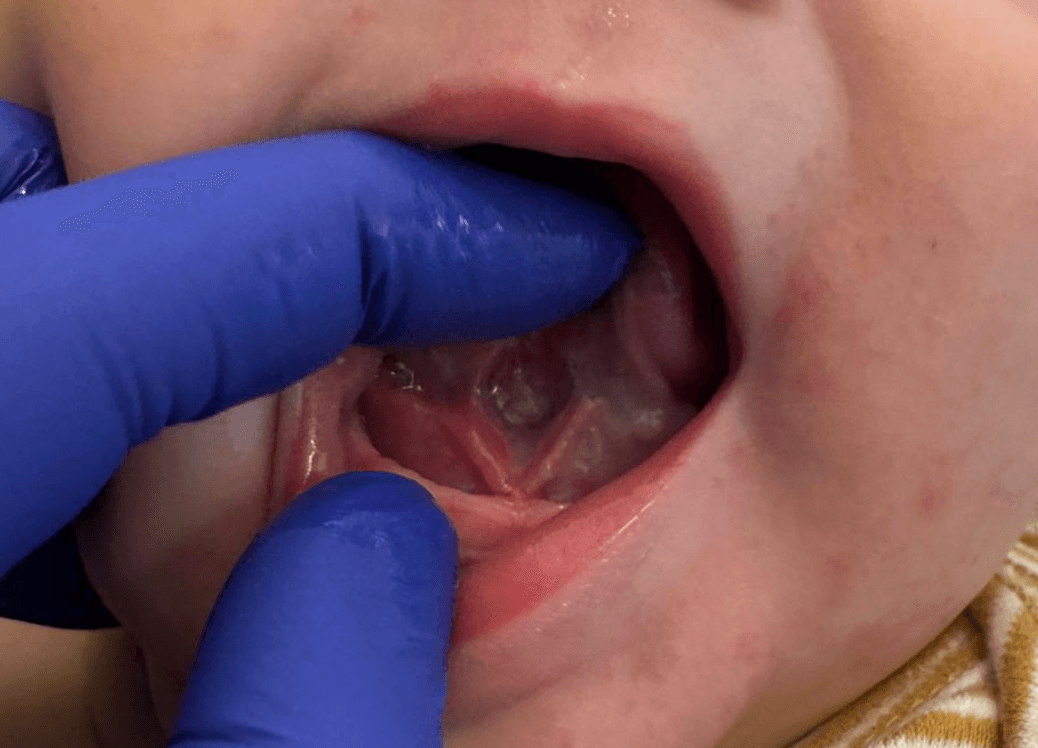
How do I know if my baby really needs a frenectomy?
The criterion is functional, not anatomical. If there is persistent maternal pain, poor weight gain, clicking sounds when nursing and clear tongue limitation that does not respond to conservative management, and a speech therapist specialised in orofacial motricity confirms the component, then we evaluate surgery. Looking at the tongue alone is not enough.
Laser or scalpel?
At Bites we use both techniques and often combine them. The diode laser cauterises as it cuts, so in babies it's almost always the better option: 1-2 minutes on tissue, minimal bleeding, no sutures, 14-20 day recovery. In thick frenula with deep muscular component we combine scissors release plus laser to seal.
Is the upper lip tie surgical?
Almost never in babies. The upper lip tie modifies on its own with maxillary growth and eruption of permanent teeth. Operating it to 'close the gap between the teeth' or 'prevent caries' has no clinical support in infants. The real indications are rare and always come from functional evaluation, not aesthetics.
What is recovery like?
With laser: mild pain, painkillers for 24-48 hours, breastfeeding resumes the same session, full healing in 14-20 days. A yellowish fibrin layer appears in the first days, this is expected. Daily speech-therapy exercises are key to prevent the scar from re-attaching.
What if my child is already 6 or older?
Yes, it can still be done. What changes is the context: we evaluate speech, swallowing, breathing and tongue posture rather than breastfeeding. The consultation involves a speech therapist and, depending on the case, an orthodontist. The technique can also vary because older children's frenula are usually more fibrous.
Have a specific case? We'd love to evaluate it together.
BOOK A VISIT